Pain, as a critical health outcome, has been extensively studied across various disciplines. However, the role of environmental stimulation in reducing patients' perceptions of pain in healthcare settings is a relatively emerging area of research. Recent studies have explored the use of environmental stimuli, such as light, nature, music, and virtual reality, as sources of distraction to alleviate pain during medical procedures. This study aims to examine the research objectives, methodologies, and findings of empirical studies in this domain, addressing the following questions: What types of research designs and methods have been employed? What instruments have been used to measure pain? What are the key findings from these studies? A systematic literature search was conducted across four major databases—PsycINFO, PubMed, Wiley Online Library, and Google Scholar—using eight keywords: ‘pain,’ ‘environment,’ ‘light,’ ‘nature,’ ‘sound,’ ‘music,’ ‘virtual reality,’ and ‘video.’ Studies were included if they were empirical, published after 2000, measured pain as a health outcome, and emphasized environmental factors. A total of 53 studies met these criteria. An analytical matrix was developed to categorize studies based on research objectives, design, sample size, methodology, and pain measurement tools. The findings were synthesized into four major themes: environmental interventions, research designs, pain measurement techniques, and outcomes. Environmental contexts included exposure to natural light (two studies), sounds of nature (one study), combined view and sound of nature (one study), music therapy (21 studies), and virtual reality (29 studies). Of the selected studies, 44 employed randomized controlled trials, eight used quasi-experimental designs, and one was descriptive correlational. Pain was measured using a variety of validated instruments, and the study provides a comprehensive list of these tools, detailing their strengths and limitations. This article offers valuable insights for future research by identifying methodological gaps, suggesting research designs that incorporate environmental stimuli, and recommending appropriate pain measurement instruments. Additionally, graphical representations of research processes, pain scale administration guidelines, and pain rating scale comparisons are included to assist researchers in designing rigorous studies. These resources are particularly useful for planning randomized controlled trials or quasi-experiments to investigate the effectiveness of environmental stimulation as a distraction for reducing pain perception in healthcare settings.
| Published in | American Journal of Applied Psychology (Volume 14, Issue 1) |
| DOI | 10.11648/j.ajap.20251401.14 |
| Page(s) | 29-51 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Pain, Environmental Stimuli, Patient, Healthcare Environment, Virtual Reality, Music Therapy, Visual Analog Scale (VAS)
Environmental Stimulation | Number of Studies |
|---|---|
Exposure to Natural Light | 2 study |
View and Sound of Nature | 1 study |
Presence of Music | 21 study |
Access to VR or Video | 29 study |
Total Number of Study | 53 study |
Type | Scale | % |
|---|---|---|
Self-Reported | 1. Visual Analogue Scale (VAS) | 31% |
2. Numerical Rating Scale (NRS) | 10% | |
3. Faces Pain Scale (FPS) | 6% | |
4. Graphic Rating Scale (GRS) | 3% | |
5. McGill Pain Questionnaire (MPQ) | 3% | |
6. Faces Pain Scale-Revised (FPS-R) | 3% | |
7. Verbal Rating Scale (VRS) | 2% | |
8. Burn Specific Pain Anxiety Scale (BSPAS) | 1% | |
9. Visual Analog Thermometer (VAT) | 1% | |
10. 5-point scale of Pain control (5P) | 1% | |
Observational | Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) | 3% |
Type | Study Design | Intervention Administration |
|---|---|---|
Randomized Controlled Groups | Two Groups | Group A: With Intervention |
Group B: Without Intervention | ||
Three Groups | Group A: With Intervention | |
Group B: Without Intervention | ||
Group C: With a different or regular Intervention | ||
Randomized Controlled Conditions | One Treatment/linear | Single Group: Without intervention, then with intervention |
Crossover Treatment | Group A: Without intervention, then with intervention | |
Group B: With intervention, then without intervention |
Process | Timing |
|---|---|
Model-1 | Before & After the Trial |
Model-2 | Only after the Trial |
Model-3 | Before and During the Trial (not after the trial) |
Model-4 | Frequently or more than Two Times during the Trial |
5P | 5-Point Scale of Pain Control |
BSPAS | Burn Specific Pain Anxiety Scale |
CHEOPS | Children’s Hospital of Eastern Ontario Pain Scale |
FPS | Faces Pain Scale |
FPS-R | Faces Pain Scale-Revised |
GRS | Graphical Rating Scale |
HADS | Hospital Anxiety and Depression Scale |
MT | Music Therapy |
MPQ | McGill Pain Questionnaire |
NRS | Numerical Rating Scale |
VAS | Visual Analog Scales |
VAT | Visual Analog Thermometer |
VR | Virtual Reality |
VRS | Verbal Rating Scale |
Study | Env. Stimuli | Research Design | Sample | Process | Instrument /Scale |
|---|---|---|---|---|---|
Walch et al. (2005) [7] | Natural sunlight to reduce pain | RCT: 2 groups. a) Housed on the “bright” side of the hospital, b) Housed on the “dim” side of the same hospital unit. | 89 patients, undergoing elective cervical and lumbar spinal surgery | The intensity of sunlight in each hospital room was measured daily and psychologic questionnaires were administered on the day after surgery and at discharge. | McGill Pain Questionnaire (MPQ) |
Diette et al. (2003) [8] | Distraction therapy with nature sights and sounds | RCT: 2 groups. a) Experiment group was exposed to intervention, b) Control group was not offered the nature scene or the sounds. | 80 adult patients, undergoing Flexible Bronchoscopy (FB) with conscious sedation. | Baseline information was collected. A natural scene mural was placed at the bedside for the experimental group, accompanied by a tape of nature sounds to be played before, during, and after the procedure. Pain was reported during the procedure, and a follow-up survey was administered on the second-day post-procedure. | A 5-point scale of Pain control: poor, fair, good, very good, or excellent |
Bernhofer et al. (2014) [9] | Light exposure to sleep-wake patterns, mood, pain | A descriptive correlational design | 23 women and 17 men were admitted to a hospital | Medical inpatients were exposed to light levels that were insufficient for circadian entrainment. Over 72 hours, light exposure and sleep-wake patterns were continuously measured with wrist actigraph/light meters for each participant. Mood was measured daily using the Profile of Mood States BriefTM Form. Subjective pain scores were abstracted from medical records. | Numerical Rating Scale (NRS) of 0-10 with 0 being no pain and 10 being worst pain |
Aragon et al. (2002) [10] | A single 20-minute live harp playing session on patient anxiety, pain, and satisfaction | A prospective, quasi-experimental, and repeated measures design was used. A single-treatment study. | 17 patients who were postoperative and admitted to a hard-wired-bedside-monitored room of the Vascular Thoracic Unit | The VAS was completed 5 minutes before, immediately after, and 10 minutes following the 20-minute harp-playing session. Patient satisfaction was assessed using a 4-item questionnaire. Physiological measures (heart rate, systolic and diastolic blood pressure, etc.) were recorded from the bedside monitor at baseline (5 minutes before setup), at the start, and at 5, 10, 15, and 20 minutes during the harp session, as well as 5 and 10 minutes post-session. | Visual analog scales (VAS) for pain & anxiety. Physiological measures were recorded from the bedside monitor |
Kwekkeboom (2003) [11] | a) Music is better than simple distraction; b) both are better than treatment as usual | RCT: 3 groups. a) experimental music intervention, b) experimental distraction intervention c) control group of treatment as usual, | 58 people with cancer, Mean age- 53, | Pain intensity ratings were made for three time points: before, during, and post-procedure. Perceived control over pain and anxiety during and after their procedure was measured using a single-item rating created for this study. | Pain intensity by NRS. Severity of pain was rated “right now” from 0 to 10. Perceived controls by NRS (0-10) |
McCaffrey & Locsin (2006) [12] | Music on pain & acute confusion in older adults undergoing hip and knee surgery | RCT: 2 groups. a) Control group b) Experimental group | 124 patients of age 65 years or older Mean age - 75, Having elective hip or knee surgery | The experimental group had a bedside compact disc (CD) player that would automatically play the compact disc 4 times daily. Nurses’ notes, medication records, and the scores for ambulation from the physical therapy - reviewed. Each patient was called 10 days after discharge to determine his or her satisfaction. | NRS (1 to 10). Number of pain medications |
Nilsson et al. (2001) [13] | Music or music with therapeutic suggestions (M/TS) could improve recovery of hysterectomy patients. | RCT: 3 groups. a) Music group b) Music combined with therapeutic suggestions (M/TS), c) Control group exposed to operation room sounds. | 89 patients, ASA I-II, Mean age 51 years, Having an elective abdominal hysterectomy via a lower abdominal incision | Pain intensity was registered every hour for the first 24 hours and every 3 hours after 24 hours until the patient felt no pain. | Visual Analogue Scale (VAS); |
Nilsson et al. (2003)1 [14] | Music effects on postoperative pain | RCT: 3 groups. a) Listened to music intra-operatively, b) Listened to music postoperatively, c) Listened to ‘white noise’ or control group. | 151 American Society of Anaesthesiologists ASA I-II patients, aged 21-85 years, Having day-case surgery under general anesthesia | Postoperatively, the patient rated pain intensity every ½ h for 2 h in the PACU. Pain was also assessed after 1 h in the PACU, at discharge, at home in the evening of the day of surgery, days 1 and 2 after surgery in the morning and in the evening. | Numeric Rating Scale (NRS) from 0 to 10 (0-no pain to 10- maximal possible pain); Amount of morphine. |
Nilsson et al. (2003)2 [15] | Music or music with therapeutic suggestions (M/TS) could improve postoperative recovery in day-surgery. | RCT: 3 groups. a) only music, b) music in combination with therapeutic suggestions, c) Blank tape in the postoperative period. | 182 patients having varicose vein or open inguinal hernia repair surgery under general anesthesia | The surgical technique, anesthesia and postoperative analgesia were standardized. Heart rate and oxygen saturation were monitored before the intervention. Vas was measured every half hour until the patient reported < 3 on the scale. | Visual Analogue Scale (VAS); Amount of morphine |
Nilsson et al. (2005) [16] | Stress reduction and analgesia in patients exposed to calming music postoperatively | RCT: 3 groups. a) intraoperative music, b) postoperative music, c) silence or control group | 75 (ASA) Grade I-II consecutive patients, mean age 56, having surgery of open Lichtenstein inguinal hernia repair under | A 4-month period study. Anesthesia and postoperative analgesia were standardized. Pain, blood pressure, and heart rate were assessed 30 min before anesthesia and 1 hour after admission to the post-anaesthesia care unit (PACU). | NRS (0-10). Physiological Data -Blood Glucose, Blood Pressure, Pulse and amount of morphine. |
Sendelbach et al. (2006) [17] | Music therapy - physiological & psychological outcomes for patients undergoing cardiac surgery | RCT: 2 groups. a) received 20 minutes of music (N=50), b) 20 minutes of rest in bed (N=36), | 86 patients, Mean age -63.3, Having CABG or heart valve replacement. | For both groups, measures for pain intensity, HR, and BP were obtained immediately before and after each 20-minute intervention period in a consistent fashion. | NRS (0-10) Physiological data - Heart rate, Blood pressure |
Shertzer & Keck (2001) [18] | soothing music and lowering noise levels on the pain experience of patients during their PACU stay | RCT: 2 groups. a) Listened to music on a day when staff kept extraneous noise at a minimum in the PACU, b) Experienced the typical PACU day | 97 patients, Mean age 59. Undergoing same-day surgery from all surgery services except the open heart. | Pain intensity data were collected at 3 time intervals: on admission to the PACU, 30 minutes after admission, and at discharge. The 30-minute time period was chosen because patients typically remained in the PACU for 1 hour, and 30 minutes would be the midpoint of their stay. | 11-point Numerical Rating Scale (NRS), or by a Narrative questionnaire of 0 to 11 points. |
Voss et al. (2004) [19] | Sedative music reduces anxiety and pain during chair rest after open-heart surgery | RCT: 3 groups. a) Sedative music (N=19), b) Scheduled rest (N=21), c) Treatment as usual (N=21) | 61 adult postoperative open-heart surgery patients who were ordered to chair rest. | 30-minute session for all three groups during chair rest. Pain sensation and distress were measured with VAS at the initiation of chair rest and after 30 30-minute sessions. VAS took 30 to 60 seconds to present and complete. | Pain Sensation VAS; Pain Distress VAS; |
Yilmaz et al. (2003) [20] | Music on sedation in extracorporeal shock wave lithotripsy (ESWL) treatment to compare its anxiolytic effects with those of midazolam. | RCT: 2 groups. a) 2 mg of midazolam was administered intravenously 5 minutes before ESWL. Had a headset without music. b) music chosen by the patients was listened to with a headset and continued during the treatment. | 98 patients, aged 19 to 68 years, With urolithiasis in ASA I-II status and had only one urinary trackstone. | All the physiological status was recorded as baseline information. VAS was measured at 1st minute and every 10 minutes. | VAS, Physiological data - Hemodynamic parameters, Mean arterial pressure, Heart rate, respiration rate, and oxygen saturation. |
Zimmerman et al. (2006) [21] | Music & music video intervention on pain and sleep in 2nd & 3rd postoperative day | RCT: 3 groups. a) Music therapy, b) Music video therapy, c) Scheduled rest period or comparison group. | 96 patients, Mean Age -67, Having Coronary Artery Bypass Graft (CABG) surgery | MPQ & VRS were administered for baseline information. Each day had two 30-minutes sessions. VRS obtained before and after each session. MPQ was administered before session 1 and after session 4. | Verbal Rating Scale (VRS), McGill Pain Questionnaire (MPQ), |
Allred et al. (2017) [22] | Listening to music or having a quiet rest period just before and after the first ambulation can reduce pain and/or anxiety | RCT: 2 groups. a) music intervention group (Listening to music using headphones) b) quiet rest group | 56 patients (M-25 & F-31), age range 46 to 84 years, mean age 63.89. | 56 patients undergoing total knee arthroplasty were randomly assigned to either a music intervention group or a quiet rest group. The intervention took place on Postoperative Day 1, with patients listening to music for 20 minutes both before and after their first ambulation. | VAS (T1, T2, T3, T4) |
Antall and Kresevic (2004) [23] | A guided imagery intervention in the older adult patient who underwent joint replacement surgery. | RCT: 2 groups. a) usual care and a guided imagery audiotape intervention. b) usual care and a music audio tape | 13 patients (M-13), mean age 67.85 years, diagnosed with Osteoarthritis. | The experimental group received guided imagery using headphones twice a day for 20 minutes, beginning the evening after surgery and continuing until discharge. The control group received usual care with a music audio tape. | VAS (post operation, day 1) |
Chen et al. (2015) [24] | music could lower pain intensity and opioid dosage during postoperative days. | RCT: 2 groups. a) music group b) control group | 56 patients (M-10 & F-20), age range 45 to 85 years, mean age 68 years. Patients who underwent total knee replacements | The experimental group listened to soothing piano music and Chinese violin music at the following times: 1) 30 minutes the night before the operative day, 2) 30 minutes while waiting for the operation, and 3) 60 minutes in the postoperative recovery (POR). | VAS (post operation) and Opioid dosage |
Finlay et al. (2016) [25] | To examine the effect of harmony and rhythm on acute, post-operative pain of patients scheduled for knee surgery | RCT: 5 groups. a) four music listening group b) control group | 98 patients (M-40 & F-58), mean age 68 years, diagnosed with arthritic pain, radiographic Arthritis. | After surgery using standardized anesthesia, participants undertook a 15-minute intervention per day of in-patient stay. Measures of pain intensity, pain interference, salivary cortisol concentration, and mood were obtained. | VRS, NRS, Short-Form McGill Pain Questionnaire, Brief Pain Inventory. |
Gallagher et al. (2018) [26] | MT sessions on post-elective orthopedic surgery patients' pain, mood, nausea, anxiety, use of narcotics and antiemetics, and length of stay. | RCT: 2 groups. a) experimental group - music therapy b) control group - standard medical care | 163 patients, (M-92 & F-71), mean age 60.5 years, diagnosed with Osteoarthritis and going through Surgery (Knee 69, hip 88, and shoulder 6) | Patients received music therapy within 24 hours of admission to the unit, as well as every day of their stay. Same-day pre- and post-intervention data were collected 30 minutes apart for both groups, including patient self-reported mood, pain, anxiety, and nausea. Medication use and length of stay were obtained from the electronic medical record. | Numerical Rating Scale (NRS) |
Masuda et al. (2005) [27] | To examine the effect of music listening on postoperative pain and/or stress in elderly orthopedic patients. | RCT: 2 groups. a) experimental group - music therapy (M) b) control group - standard medical care (C) | 44 (M-18 & F-26), age range 60 to 89 years, mean age 69 years. Diagnosed with spinal disorders: joint disorders (24), musculoskele (16), tal tumors (2), trauma (2) | The patients in Group M were given the option to listen to music for 20 minutes in private rooms. Pain levels were evaluated using the Visual Analog Scale (VAS) and the Wong-Baker Faces Scale (FS). As indicators of stress, systolic and diastolic blood pressure, heart rate, skin temperature, and fingertip blood flow were measured. | Visual Analogue Scale (VAS) Wong/Baker Faces Scale (FS) |
Mondanaro et al. (2017) [28] | To examine the effect of music therapy (MT) interventions on the recovery of patients after spine surgery | RCT: 2 groups. a) experimental group - MT plus standard care (medical and nursing care with scheduled pharmacologic pain intervention) b) control group - standard care only | 60 patients (M-25 & F-35), age range 40 to 55 years | Measurements for both groups were taken before and after the intervention. MT used patient-preferred live music to promote relaxation through improvisation, singing, rhythmic drumming, or guided visualization. Patients listened to music for 30 minutes postoperatively. The control group received earbuds and standard care. | visual analog scale (VAS) VAS (pre, post operation) Hospital Anxiety and Depression Scale (HADS) Tampa scale |
Simcock et al. (2008) [29] | To examine the effect of patient-selected music on reducing perceived pain | RCT: 2 groups. a) experimental group - music therapy 9M) b) control group - standard medical care (C) | 30 patients (M-12 & F-18), Mean age 67.3 years, diagnosed with Osteoarthritis (26), traumatic arthritis (2), rheumatic arthritis (1), or lupus (1) | The experimental group wore headphones and MP3 players, listening to music selected by the patient during the surgical procedure. For the control group, a blank file was played during the procedure. VAS was administered preoperatively and at 3, 6, and 24 hours postoperatively. | VAS |
Saadatmand et al. (2015) [30] | Natural sounds may help reduce the potentially harmful effects of anxiety and pain in hospitalized patients | RCT: 2 groups. a) Experimental group (n=30) b) Control group (n=30) | 60 patients who are receiving mechanical ventilation support. | All participants wore headphones for 90 minutes. The intervention group heard pleasant natural sounds, while the control group heard nothing. Outcome measures included self-reported VAS for pain at baseline, 30, 60, and 90 minutes into the intervention, and 30 minutes after. | Visual Analog Scale (VAS) |
Chan et al. (2007) [31] | Usability and effectiveness of VR in reducing pain in wound-care procedures for pediatric burn patients | RCT: 2 groups. a) Control b) Experiment. Each patient participated in a single VR trial: once with VR and once without VR. | 8 eligible patients: Mean age is 6.54. 7 had been scalded and 1 had been burned. | a) Children reported FPS before, during, and after, b) Interview with nurses, c) Nurses conduct the usability and modified presence questionnaires (PQ), d) A Semi-structured interview for 15 minutes with nurses about their perception of PQ. | Faces Pain Scale (FPS) from 0-100; Usability and modified presence questionnaires (PQ) |
Das et al. (2005) [32] | VR game to decrease procedural pain in children (5 - 18 years) with acute burn injuries. | RCT: 2 groups. a) routine pharmacological analgesia, or b) routine pharmacological analgesia with VR | 7 Children (5 - 18 years), having burns to more than 3% of their body surface area, & requiring dressing changes | Dressing change has two phases. The subjects were asked to score their average pain experience at the end of each phase of the dressing change procedure. An interview with the child, mother, and the nursing staff. | Self-report FPS 0 (No Hurt) to 10 (Very bad/Worst Hurt) |
Gershon et al. (2003) [33] | VR to alleviate pain and anxiety associated with an invasive procedure for a pediatric cancer patient | Single Case Study. Control condition: No distraction (A), non-VR distraction on a computer screen (B), and VR distraction with a headset (C). | An 8-year-old Caucasian male with a diagnosis of acute lymphocytic leukemia, received more than 10 previous port accesses. | A-B-C-A design during four consecutive appointments. The child, parents, and nurse gave VAS pain and anxiety ratings before and after each port access. CHEOPs were recorded during the procedure (5-10 min long procedure). Pulse rate monitored before, during, and after. | VAS (10-cm) line with a slide ruler with facial depictions to help the child. CHEOPS; Pulse rate. |
Gershon et al. (2004) [34] | VR as a distraction for children with cancer | RCT: 3 groups a) VR distraction (n=22), b) No distraction control group (n=22), c) Non-VR distraction | 59 children, Mean age - 12.7. Having a diagnosis of childhood cancer. | Parents, children, and nurses assessed the child’s pain at two intervals; before the port access procedure and after it was completed. Pulse rate was monitored 3 times; before, during, and after. Researched recorded CHEOPS during the procedure. | VAS; CHEOPS; Pulse Rate; |
Gold et al. (2006) [35] | VR as a pain distraction for pediatric intravenous (IV) placement for an MRI or CT scans | RCT: 2 groups. a) VR distraction using Street Luge (5DT), presented via a head-mounted display, or (2) standard of care (topical anesthetic) with no distraction. | 20 children, Mean age - 10.2, Requiring IV placement for MRI or CT scans that required IV placement. | Following the screening tasks, children and their parents completed baseline measures. Participants completed self-report surveys at 3 separate intervals: approximately 30 min before the IV, immediately before the IV, and following IV placement. | VAS Wong-Baker FACES Pain Rating Scale Faces Pain Scale-Revised to assess affective pain |
Hoffman et al. (2000) [36] | VR to distract patients from pain during physical therapy for burn patients. | Quasi-experiment, One-treatment RCT: 2 conditions a) 3 minutes with no distractions, or b) 3 minutes in VR distraction. | 12 patients average of 21% of total body surface area burned, mean age - 27.6, Performed range of motion exercises of their injured extremity under an occupational therapist. | Pain was measured after each 3 minutes of experimental treatment during a brief pause in physical therapy. At each pause, patients completed five retrospective subjective pain ratings using 100-mm VASs. With respect to the last 3 minutes of physical therapy, patients rated the variable; Spent thinking about their pain, worst pain, and average pain. | 100-mm VAS pain ratings Scale for pain variables. |
Hoffman et al. (2001)1 [37] | Immersive VR continues to reduce pain (via distraction) with repeated use. | RCT: 2 groups. a) VR condition b) Control condition. | 17 patients average of 23.7% total body surface area burned. Mean age - 21.9; performed range-of-motion exercises under an occu-therapist. | Each 3-day period had two sessions (VR and Control). The mean VR durations were 3.5, 4.9, and 6.4 minutes. Patients completed assessments during a brief 2-minute pause after each treatment. | Five VAS -retrospective subjective pain ratings with use 100-mm VAS. |
Hoffman et al. (2001)2 [38] | VR can serve as an effective non-pharmacologic analgesic for dental pain | Case study - 2 people. One treatment 3 conditions: a) VR distraction, b) Movie distraction, c) No-distraction | 2 patients (aged 51 and 56 years old) Receiving periodontal scaling & root planning | Patient 1 spent 2.5 minutes, and Patient 2 spent 5 minutes in each of the 3 treatment conditions. Pain ratings were collected after each treatment during a 2-minute pause in dental care. After each pause (following VR, movie watching, and no distraction), patients completed retrospective pain ratings. | VAS pain scores using 0-10 scales; |
Hoffman et al. (2004) [39] | Water-friendly VR technology with a burn patient undergoing wound care in a hydrotherapy tub. | Quasi-Experiment Single case study. Two condition: a) Spent 3 minutes of the procedure in VR, b) 3 minutes with no distraction. | A 40-year-old male with 19% total body surface area deep flame/flash burns to his legs, neck, back, and buttocks. | The patient was given analgesic medication for procedural pain. Pain and presence ratings were administered after each treatment condition during a brief pause in wound care, with the patient completing several 10-point scale ratings. After wound care, the patient answered some questions. | Graphical Rating Scale (GRS) |
Hoffman et al. (2005) [40] | VR as an adjunctive pain control during Transurethral Microwave Thermotherapy (TUMT) for elderly patient | Quasi-Experiment - Single case study | A 67-year-old man with BPH, previous bladder stones, and obstruction requiring intermittent catheterization presented for TUMT. | Once the mid-intraprostatic temperature reached 50°C, the patient answered pain questions and completed the VAS based on the last 2 minutes. The questionnaire was repeated after 3 minutes and again at 3 and 10 minutes following VR immersion. The total treatment lasted 37.5 minutes. | A validated, standardized pain questionnaire consisting of five questions with a 10-point VAS. |
Hoffman et al. (2008) [41] | The adjunctive use of water-friendly immersive VR to distract patients from their pain during burn wound debridement in the hydro tank. | RCT: One treatment 2 conditions study. a) 3 minutes with no distraction, b) 3 minutes in VR distraction. | 11 hospitalized inpatients, (9 to 40 years) Mean age - 27, had their burn wounds debrided and dressed while partially submerged in the hydrotank. | Standard analgesics were given 30 to 45 minutes before the procedure. A 6-minute segment of wound care was conducted under two conditions. During two brief pauses (after each 3 minutes), patients completed three subjective pain ratings for the preceding 3 minutes of wound care. | Three 0 to 10 GRS pain scores (worst pain, time spent thinking about pain, and pain unpleasantness) for each of the 2 treatment conditions |
Patterson et al. (2004) [42] | A 3-D immersive, VR world as a means to control pain & anxiety to a severely burn patient | A quasi-experiment with a single case study involved a two-day treatment under two conditions: Day 1 used hypnotic induction with a 3D VR world, and Day 2 used hypnotic induction without VR, instructing the patient to imagine entering the 3D canyon. | A 37-year-old male, admitted for burns that covered 55% of the patient’s total body surface area. | On Day 40, the patient rated baseline pain. On Day 1, the patient began wound care 2 hours after a 90-minute VR hypnotic induction. Pain ratings were administered immediately after by a research assistant. On Day 2, wound care began 1 hour after the intervention, with no psychological intervention during the session. After returning to his room, the patient completed pain and anxiety ratings with the research assistant. | GRS; Burn Specific Pain Anxiety Scale (BSPAS); |
Steele et al. (2003) [43] | VR may serve as a powerful non-pharmacologic analgesic for children following surgery | Quasi-Experiment with a single Case study. A within-subject design in 2 conditions; a) VR with usual pharmacologic analgesics, b) No VR with usual pharmacologic analgesics. | One 16-year-old boy who had Single Event Multi-Level Surgery | Daily two sessions of physiotherapy from post-operative day 2 to day 6. Patient spent half of the session (approximately 10 min) using VR and half without VR. The patient was asked to rate his pain twice during each physiotherapy session: after the VR and the no-VR conditions. | A self-reported FACES scale was altered to facilitate the use of the scale with the SEMLS population. 1 to 5 scale. |
Van et al. (2007) [44] | VR can reduce the procedural pain and anxiety during burn wound care session | RCT: 3 groups. a) standard care (no distraction), b) VR distraction, c) Another self-chosen distraction; television, music, non-medical conversation, and distraction by a childcare worker. | 19 inpatients ages 8 to 65 years (mean, 30 years) with a mean TBSA of 7.1% (range, 0.5-21.5%) | Each patient received the standard analgesic regimen. VR was provided during one wound dressing change in the first week, with standard care or alternative distraction on other days. A nurse recorded VAT pain scores the day before VR (no distraction), the day of VR, and the day after VR (no distraction). | Pain - Visual Analog Thermometer (VAT); Anxiety - the state-version of the Spielberger State-Trait Anxiety Inventory. |
Wint et al. (2002) [45] | To examine the effects of VR glasses as a non-pharmacologic aid for cancer patients undergoing frequent lumbar punctures. | A Pilot study. RCT: 2 groups. a) Standard intervention during the LP, b) Standard intervention with VR glasses and watching a video (experimental). | 30 adolescents with cancer (17 in the VR and 13 in the control group) undergoing frequent Lumbar Punctures (LPs). | After the LP, the nurse assessed sedation using the Sedation Assessment Scale. Both groups marked their pain level on the VAS, and patients were interviewed about their experience. | VAS; Usability Sedation Assessment Scale. |
Wolitzky et al. (2005) [46] | VR is a behavioral intervention designed to decrease distress when receiving treatment for cancer and undergoing a port access procedure | RCT: 2 groups. a) VR condition, b) No VR treatment as a control condition. | 20 children ages 7 to 14 receiving treatment for cancer and undergoing a port access procedure. 12 male, 55% African-American, 40% White, and 5% Asian. | After the session, the researcher conducted How-I-Feel Questionnaire for the child. The pulse monitor was then connected to the child’s finger. The VAS ratings, parents, children, and the nurse all rated the child’s pain and anxiety on a 0-100 scale before and during the procedure. A composite measure of distress before and during the procedure. | How-I-Feel questionnaire; Pulse rate; VAS for pain; Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS); |
Mohammad and Ahmad, (2019) [47] | Immersive Virtual Reality (VR) | RCT: 2 groups. a) VR condition, b) No VR. | 80 Female patients with breast cancer, average age of 51.99 | For the VR group, assessment was conducted before giving the morphine and after finishing the VR session (VR started exactly at the peak time effect for 15 minutes). For the control group (no VR) assessment was conducted just before giving the morphine and at 15 minutes after the peak time effect. | A visual analog scale (VAS) to measure pain (a 10-cm scale) |
Ding et al, (2019) [48] | To examine the effects of Immersive Virtual Reality (VR) in patients who had undergone hemorrhoidectomy during the dressing change | RCT: 2 groups. a) VR condition and standard pharmacological analgesic intervention b) No VR, a control condition (standard pharmacological analgesic intervention). | 182 patients (M-72 & F-110, mean age-45.82. Patients who had undergone hemorrhoidectomy | Pain scores and physiological measurements were collected before, during, and after the first postoperative dressing change. The standard dressing change procedure consisted of removing the dressings, cleaning and sterilizing the wound, wound assessment, and covering the wound with a new dressing. | The VAS referred to a 10-cm visual scale representing a continuum with the ends marked ‘0 (no pain)’ and ‘10 (unbearable pain)’ |
Chan et al, (2019) [49] | To assess the efficacy and safety of a VR distraction for needle pain in an emergency department (ED) and an outpatient pathology (ie, outpatient laboratory). | RCT: 2 groups. 2 clinical trials. It randomized undergoing venous needle procedures to virtual reality or the control was standard of care (SOC) practice. | 123 patients children aged 4-11 years, mean -8.2 (M-74 & F -55). Populations in whom needle procedures are commonly performed. | In the ED, 64 children were assigned to virtual reality and 59 to SOC. In pathology, 63 children were assigned to virtual reality and 68 to SOC; 2 children withdrew assent in the SOC arm, leaving 66. Pain was measured for baseline pain between virtual reality and SOC on child-rated Faces Pain Scale-Revised. | Child-rated Faces Pain Scale |
Dumoulin et al, (2019) [50] | To examine the efficacy of VR as a mode of distraction during a medical procedure compared with two conditions. | RCT: 3 groups. A) VR, B) watching TV with minimal control C) distraction provided by the Child Life gold standard control program | 59 children (8-17 years, mean 13.37), Male -38 and Female -21. Children were recruited through the emergency department | A total of 59 children were randomly assigned to one of the three conditions. pain intensity and fear of pain were measured using VAS before and right after the procedure. Patient satisfaction was measured after the intervention. | A visual analog scale (VAS) |
Alshatrat et al, (2019) [51] | To identify the effect of immersive VR on pain perception during scaling and root planning procedures (SRP) in dental hygiene clinics. | RCT: 2 groups a) without VR condition, or b) with VR condition. | 50 patients, male-22 and female-28, average age of 36.84, who need dental hygiene. | Within-subject/split-mouth design was used in this study. The participants received a full mouth SRP. Pain was measured by VAS. Participants were also asked three questions to assess presence, realism, and nausea. | Visual Analog Scale (VAS): 0-10 scales with cut points on the scale indicating that (0) none, (1-3) mild, (4-6) moderate or (7-10) severe. |
Rothgangel et al, (2018) [52] | To compare the effects of traditional mirror therapy (MT), a patient-centered tele-treatment (PACT), and sensomotor exercises without a mirror on phantom limb pain (PLP). | RCT: Three conditions: a) traditional MT followed by a tele-treatment using augmented reality MT, b) traditional MT followed by self-delivered MT, c) sensomotor exercises of the intact limb without a mirror followed by self-delivered exercises. | 75 patients (M-52 & F-23, mean - 61.12). Adult patients with unilateral lower limb amputation and average PLP intensity of at least 3 on the 0-10 Numeric Rating Scale (NRS). | Subjects randomly received any of the three conditions for four weeks. Intensity, frequency, and duration of PLP and patient-reported outcomes assessing limitations in daily life at baseline, 4 weeks, 10 weeks, and 6 months. Among 75, traditional MT (n = 25), tele-treatment (n = 26) or sensomotor exercises (n = 24). | 0-10 Numeric Rating Scale (NRS) |
Glennon et al, (2018) [53] | To determine the effects of a VR on pain and anxiety in patients undergoing the procedure. | Quasi-exper. study: a) experiment (use of VR goggles) b) control group (standard treatment). | 97 patients, mean age- 51.40; undergoing a bone marrow aspiration & biopsy procedure. | Vital signs, pain, and anxiety were measured before and after the procedure. | VAS |
Piskorz and Czub, (2018) [54] | VR technology is an effective tool in the treatment of acute pain in children with dysfunctional kidneys. | Quasi-experimental study: 2 groups - a) with VR, b) no VR | 38 patients (M-20 & F-18, mean - 11.32), children staying in hospital with dysfunctional kidneys | Participants in the treatment group received the venipuncture procedure with VR distraction. Participants rated their pain and stress intensity. | Visual analog scales (VAS) on a scale of 0 to 100. A short questionnaire. |
Gold and Mahrer, (2018) [55] | To evaluate the feasibility and efficacy of VR compared with SOC for reducing pain, and anxiety, and improving satisfaction associated with blood draw in children ages 10-21 years. | RCT: 2 groups. a) virtual reality (VR), b) standard of care (SOC) 143 triads were randomized to receive either VR or SOC when undergoing routine blood draws. | 143 triads (patients, their caregivers, and the phlebotomist). Male-72 and female-71, average age of 15.43. Patients with procedural pain | Patients and caregivers completed pre- and post-procedural measures of pain, anxiety, and satisfaction, while phlebotomists reported on the patient's experience during the procedure. Patients and caregivers used the VAS, CAS, and Faces Pain Scale to measure affective pain before and after the procedure, and assessed their anxiety with the VAS for anxiety and the Facial Affective Scale. | VAS, Colored Analogue Scale (CAS) ranging from 0 to 10 indicating to report on pain intensity pre-procedure and post-procedure. FPS-Revised |
JahaniShoorab et al, (2015) [56] | Virtual reality is an effective complementary non-pharmacological method to reduce pain during episiotomy repair. | RCT: 2 groups. a) usual treatment with VR and local infiltration (5 ml solution of lidocaine 2%) B) control group only received local infiltration | 30 primiparous parturient women having labor, average age of 24.11 | Pain was measured using the NPR Scale before, during, and after the episiotomy repair. In total there are four stages of repair. Parturient satisfaction was recorded before and after episiotomy repair. | Numeric Pain Rating Scale (0-100) |
Kim et al, (2014) [57] | To determine the effects of a VR-based yoga program on middle-aged female low back pain patients. | RCT: 2 groups. a) a physical therapy program, b) a VR-based yoga program. | 30 middle-aged female patients with chronic low back pain. (M-0 & F-30, mean age-44.33), | Patients were distributed into two programs for four weeks. A 30-minute VR-based Wii Fit yoga program or trunk stabilizing exercise was performed thrice weekly. Pain was measured using VAS before & after intervention. | VAS - A 10-cm scale marked with 1-cm increments: 0 to 10 |
Guo et al, (2015) [58] | To assess the effect of VR distraction on pain among patients with a hand injury undergoing a dressing change. | RCT: 2 groups. a) experiment (49 cases), and b) control (49 cases) | 98 patients, Male-85 and Female -13. Hand injury (including cuts nail bed damage or skin avulsion) | Pain levels were compared between the two groups before and after the dressing change using a visual analog scale (vas). | VAS |
Brown et al, (2014) [59] | Investigate the effect of the Ditto™ intervention on re-epithelialization rates in acute pediatric burns. | RCT: 2 groups. a) Ditto™ Group, b) Control Group (standard) | N=75 (M-60 & F-39) children (4-12 years, mean -8.33) with an acute burn. | Burn re-epithelialization, pain intensity, anxiety and stress measures were obtained at every dressing change until complete wound re-epithelialization. | FPS-R, FLACC, VAS-A |
| [1] | International Association for the Study of Pain, IASP. (1995) Pain Measurement in Children. Pain Clinical Updates, 3(2). |
| [2] | International Association for the Study of Pain, IASP. (2020). Definition of pain. In: Terminology. Available online at: |
| [3] | Melzack R, Wall PD. (1965). Pain mechanisms: a new theory. Science, 150: 971-979. |
| [4] | McCaul KD, Malott JM (1984). Distraction and coping with pain. Psychol Bull, 95: 516-533. |
| [5] | Mahrer, NE. and Gold, JI. (2009). The Use of Virtual Reality for Pain Control: A Review. Current Pain and Headache Reports, 13: 100-109. |
| [6] | Malenbaum, S., Keefe, FJ., Williams, ACdeC, Ulrich, R. and Somers, TJ. (2008). Pain in its environmental context: Implications for designing environments to enhance pain control. Pain, 134(3): 241-244. |
| [7] | Walch JM, Rabin BS, Day R, Williams JN, Choi K, Kang JD. (2005). The effect of sunlight on postoperative analgesic medication use: a prospective study of patients undergoing spinal surgery. Psychosom Med, 67: 156-63. |
| [8] | Diette GB, Lechtzin N, Haponik E, Devrotes A, Rubin HR. (2003). Distraction therapy with nature sights and sounds reduces pain during flexible bronchoscopy: a complementary approach to routine analgesia. Chest, 123: 941-8. |
| [9] | Bernhofer, E. I., Higgins, P. A., Daly, B. J., Burant, C. J., & Hornick, T. R. (2014). Hospital lighting and its association with sleep, mood and pain in medical inpatients. Journal of Advanced Nursing, 70(5), 1164-1173. |
| [10] | Aragon D., Farris C. and Byers J. F. (2002). The effects of harp music in vascular and thoracic surgical patients. Alternative Therapies in Health and Medicine, 8(5): 52. |
| [11] | Kwekkeboom KL. (2003). Music versus distraction for procedural pain and anxiety in patients with cancer. Oncol Nurs Forum, 30(3): 433-440. |
| [12] | McCaffrey R, Locsin R. (2006). The effect of music on pain and acute confusion in older adults undergoing hip and knee surgery. Holist Nurs Pract. 20(5): 218-226. |
| [13] | Nilsson U, Rawal N, Uneståhl LE, Zetterberg C, Unosson M. (2001). Improved recovery after music and therapeutic suggestions during general anaesthesia: a double-blind randomised controlled trial. Acta Anaesthesiol Scand. 45(7): 812-817. |
| [14] | Nilsson U, Rawal N, Unosson M. (2003). A comparison of intra-operative or postoperative exposure to music- a controlled trial of the effects on postoperative pain. Anaesthesia. 58(7): 699-703. |
| [15] | Nilsson U, Rawal N, Enqvist B, Unosson M. (2003). Analgesia following music and therapeutic suggestions in the PACU in ambulatory surgery; a randomized controlled trial. Acta Anaesthesiol Scand, 47(3): 278-283. |
| [16] | Nilsson U, Unosson M, Rawal N. (2005). Stress reduction and analgesia in patients exposed to calming music postoperatively: a randomized controlled trial. Eur J Anaesthesiol. 22(2): 96-102. |
| [17] | Sendelbach SE, Halm MA, Doran KA, Miller EH, Gaillard P. Effects of music therapy on physiological and psychological outcomes for patients undergoing cardiac surgery. J Cardiovasc Nurs. 2006; 21(3): 194-200. |
| [18] | Shertzer KE, Keck JF. (2001). Music and the PACU environment. J Perianesth Nurs. 16(21): 90-102. |
| [19] | Voss, J. A., Good, M., Yates, B., Baun, M. M., Thompson, A., & Hertzog, M. (2004). Sedative music reduces anxiety and pain during chair rest after open-heart surgery. Pain, 112(1-2), 197-203. |
| [20] | Yilmaz E, Ozcan S, Basar M, Basar H, Batislam E, Ferhat M. (2003). Music decreases anxiety and provides sedation in extracorporeal shock wave lithotripsy. Urology. 61(2): 282-286. |
| [21] | Zimmerman L, Nieveen J, Barnason S, Schmaderer M. (1996) The effects of music interventions on postoperative pain and sleep in coronary artery bypass graft (CABG) patients. Sch Inq Nurs Pract, Summer; 10(2): 153-70. |
| [22] | Allred, K. D., Byers, J. F., & Sole, M. L. (2010). The effect of music on postoperative pain and anxiety. Pain Management Nursing, 11(1), 15-25. |
| [23] | Antall, G. F., & Kresevic, D. (2004). The use of guided imagery to manage pain in an elderly orthopaedic population. Orthopaedic Nursing, 23(5), 335-340. |
| [24] | Chen, H. J., Chen, T. Y., Huang, C. Y., Hsieh, Y. M., & Lai, H. L. (2015). Effects of music on psychophysiological responses and opioid dosage in patients undergoing total knee replacement surgery. Japan J. of Nursing Science, 12(4), 309-319. |
| [25] | Finlay, K. A., Wilson, J. A., Gaston, P., Al-Dujaili, E. A., & Power, I. (2016). Post-operative pain management through audio-analgesia: Investigating musical constructs. Psychology of Music, 44(3), 493-513. |
| [26] | Gallagher, L. M., Gardner, V., Bates, D., Mason, S., Nemecek, J., DiFiore, J. B.,. & Bethoux, F. (2018). Impact of music therapy on hospitalized patients post-elective orthopaedic surgery: a randomized controlled trial. Orthopaedic Nursing, 37(2), 124-133. |
| [27] | Masuda, T., Miyamoto, K., & Shimizu, K. (2005). Effects of music listening on elderly orthopaedic patients during postoperative bed rest. Nordic Journal of Music Therapy, 14(1), 4-14. |
| [28] | Mondanaro JF, Homel P, Lonner B, Shepp J, Lichtensztein M, Loewy JV. (2017). Music Therapy Increases Comfort and Reduces Pain in Patients Recovering From Spine Surgery. Am J Orthop (Belle Mead NJ). Jan/Feb; 46(1): E13-E22. |
| [29] | Simcock, X. C., Yoon, R. S., Chalmers, P., Geller, J. A., Kiernan, H. A., & Macaulay, W. (2008). Intraoperative music reduces perceived pain after total knee arthroplasty-A blinded, prospective, randomized, placebo-controlled clinical trial. The journal of knee surgery, 21(04), 275-278. |
| [30] | Saadatmand, V., Rejeh, N., Heravi-Karimooi, M., Tadrisi, S. D., Vaismoradi, M., & Jordan, S. (2015). Effects of natural sounds on pain: A randomized controlled trial with patients receiving mechanical ventilation support. Pain Management Nursing, 16(4), 483-492. |
| [31] | Chan EA, Chung JW, Wong TK, et al. (2007). Application of a virtual reality prototype for pain relief of pediatric burn in Taiwan. J Clin Nurs, 16: 786-793. |
| [32] | Das DA, Grimmer KA, Sparon AL, et al. (2005). The efficacy of playing a virtual reality game in modulating pain for children with acute burn injuries: a randomized controlled trial. BMC Pediatr, 5: 1-10. |
| [33] | Gershon J, Zimand E, Lemos R, et al. (2003). Use of virtual reality as a distracter for painful procedures in a patient with pediatric cancer: a case study. Cyberpsychol Behav, 6: 657-662. |
| [34] | Gershon J, Zimand E, Pickering M, et al. (2004). A pilot and feasibility study of virtual reality as a distraction for children with cancer. J Am Acad Child Adolesc Psychiatry, 43: 1243-49. |
| [35] | Gold J, Kim S, Kant A, et al. (2005). Effectiveness of virtual reality for pediatric pain distraction during IV placement. Cyberpsychol Behav, 9: 207-212. |
| [36] | Hoffman HG, Patterson DR, Carrougher CJ (2000). Use of virtual reality for adjunctive treatment of adult burn pain during physical therapy: A control study. Clin J Pain, 16: 244-250. |
| [37] | Hoffman HG, Garcia-Palacios A, Patterson DR, et al. (2001). The effectiveness of virtual reality for dental pain control: a case study. Cyberpsychol Behav, 4: 527-535. |
| [38] | Hoffman HG, Patterson DR, Carrougher CJ, Sharar SR (2001). Effectiveness of virtual reality-based pain control with multiple treatments. Clin J Pain, 17: 229-235. |
| [39] | Hoffman HG, Patterson DR, Magula J, et al. (2004). Water-friendly virtual reality pain control during wound care. J Clin Psychol, 60: 189-195. |
| [40] | Hoffman, HG. and Wright, JL. (2005). Virtual reality as an adjunctive pain control during transurethral microwave thermotherapy. Urology, 66(6): 1320e1-1320e3. |
| [41] | Hoffman HG, Patterson DR, Seibel E, et al. (2008). Virtual reality pain control during burn wound debridement in the hydrotank. Clin J Pain, 24: 299-304. |
| [42] | Patterson DR, Tininenko JR, Schmidt AE, Sharar SR. (2004). Virtual reality hypnosis: a case report. Int J Clin Exp Hypn, 52: 27-38. |
| [43] | Steele E, Grimmer K, Thomas B, et al. (2003). Virtual reality as a pediatric pain modulation technique: a case study. Cberpsychol Behav, 6: 633-638. |
| [44] | van Twillert B, Bremer M, Faber AW (2007). Computer-generated virtual reality to control pain and anxiety in pediatric and adult burn patients during wound dressing changes. J Burn Care Res, 28: 694-702. |
| [45] | Wint S, Eshelman D, Steele J, Guzetta CE (2002). Effects of distraction using virtual reality glasses during lumbar punctures in adolescents with cancer. Oncol Nurs Forum, 29: 8-15. |
| [46] | Wolitzky, K., Fivush, R., Zimand, E., Hodges, L., Rothbaum, B. O. (2005). Effectiveness of virtual reality distraction during a painful medical procedure in pediatric oncology patients. Psychology and Health, 6: 817-24. |
| [47] | Mohammad, E. B., & Ahmad, M. (2019). Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: a randomized control trial. Palliative & supportive care, 17(1), 29-34. |
| [48] | Ding, J., He, Y., Chen, L., Zhu, B., Cai, Q., Chen, K., & Liu, G. (2019). Virtual reality distraction decreases pain during daily dressing changes following haemorrhoid surgery. Journal of International Medical Research, 47(9), 4380-4388. |
| [49] | Chan, E., Hovenden, M., Ramage, E., Ling, N., Pham, J. H., Rahim, A.,. & Leong, P. (2019). Virtual reality for pediatric needle procedural pain: two randomized clinical trials. The Journal of pediatrics, 209, 160-167. |
| [50] | Dumoulin, S., Bouchard, S., Ellis, J., Lavoie, K. L., Vézina, M. P., Charbonneau, P.,. & Hajjar, A. (2019). A randomized controlled trial on the use of virtual reality for needle-related procedures in children and adolescents in the emergency department. Games for Health Journal, 8(4), 285-293. |
| [51] | Alshatrat, S. M., Alotaibi, R., Sirois, M., & Malkawi, Z. (2019). The use of immersive virtual reality for pain control during periodontal scaling and root planing procedures in dental hygiene clinic. International Journal of Dental Hygiene, 17(1), 71-76. |
| [52] | Rothgangel, A., Braun, S., Winkens, B., Beurskens, A., & Smeets, R. (2018). Traditional and augmented reality mirror therapy for patients with chronic phantom limb pain: results of a three-group, multicentre single-blind randomized controlled trial. Clinical Rehabilitation, 32(12), 1591-1608. |
| [53] | Glennon, C., McElroy, S. F., Connelly, L. M., Lawson, L. M., Bretches, A. M., Gard, A. R., & Newcomer, L. R. (2018). Use of virtual reality to distract from pain and anxiety. In Oncology Nursing Forum, 45(4). |
| [54] | Piskorz, J., & Czub, M. (2018). Effectiveness of a virtual reality intervention to minimize pediatric stress and pain intensity during venipuncture. Journal for Specialists in Pediatric Nursing, 23(1), e12201. |
| [55] | Gold, J. I., & Mahrer, N. E. (2018). Is virtual reality ready for prime time in the medical space? A randomized control trial of pediatric virtual reality for acute procedural pain management. Journal of Pediatric Psychology, 43(3), 266-275. |
| [56] | JahaniShoorab, N., Zagami, S. E., Nahvi, A., Mazluom, S. R., Golmakani, N., Talebi, M., & Pabarja, F. (2015). The effect of virtual reality on pain in primiparity women during episiotomy repair: a randomize clinical trial. Iranian journal of medical sciences, 40(3), 219. |
| [57] | Kim, S. S., Min, W. K., Kim, J. H., & Lee, B. H. (2014). The effects of VR-based Wii fit yoga on physical function in middle-aged female LBP patients. Journal of Physical Therapy Science, 26(4), 549-552. |
| [58] | Guo, C., Deng, H., & Yang, J. (2015). Effect of virtual reality distraction on pain among patients with hand injury undergoing dressing change. Journal of Clinical Nursing, 24(1-2), 115-120. |
| [59] | Brown, N. J., Kimble, R. M., Rodger, S., Ware, R. S., & Cuttle, L. (2014). Play and heal: randomized controlled trial of Ditto™ intervention efficacy on improving re-epithelialization in pediatric burns. Burns, 40(2), 204-213. |
| [60] | Nilsson, U. (2008). The anxiety-and pain-reducing effects of music interventions: a systematic review. AORN Journal, 87(4), 780-807. |
| [61] | Sin, W. M., & Chow, K. M. (2015). Effect of music therapy on postoperative pain management in gynecological patients: a literature review. Pain Management Nursing, 16(6), 978-987. |
| [62] | Lee, J. H. (2016). The effects of music on pain: a meta-analysis. The Journal of Music Therapy, 53(4), 430-477. |
| [63] | Santiváñez-Acosta, R., Tapia-López, E. D. L. N., & Santero, M. (2020). Music therapy in pain and anxiety management during labor: a systematic review and meta-analysis. Medicina, 56(10), 526. |
| [64] | Lin, C. L., Hwang, S. L., Jiang, P., & Hsiung, N. H. (2020). Effect of music therapy on pain after orthopedic surgery—a systematic review and meta‐analysis. Pain Practice, 20(4), 422-436. |
| [65] | Pittara, M., Matsangidou, M., Stylianides, K., Petkov, N., & Pattichis, C. S. (2020). Virtual reality for pain management in cancer: a comprehensive review. IEEE Access, 8, 225475-225489. |
| [66] | Goudman, L., Jansen, J., Billot, M., Vets, N., De Smedt, A., Roulaud, M.,. & Moens, M. (2022). Virtual reality applications in chronic pain management: systematic review and meta-analysis. JMIR Serious Games, 10(2), e34402. |
| [67] | Chuan, A., Zhou, J. J., Hou, R. M., Stevens, C. J., & Bogdanovych, A. (2021). Virtual reality for acute and chronic pain management in adult patients: a narrative review. Anaesthesia, 76(5), 695-704. |
| [68] | Chan, E., Foster, S., Sambell, R., & Leong, P. (2018). Clinical efficacy of virtual reality for acute procedural pain management: A systematic review and meta-analysis. PloS one, 13(7), e0200987. |
| [69] | Huang, Q., Lin, J., Han, R., Peng, C., & Huang, A. (2022). Using virtual reality exposure therapy in pain management: a systematic review and meta-analysis of randomized controlled trials. Value in Health, 25(2), 288-301. |
| [70] | Martiny, K. (2004). Adjunctive Bright Light in Non-Seasonal Major Depression. Acta Psychiatr Scand, 110: 7-28. |
| [71] | Beauchemin, K. M., Hays, P. (1996). Sunny hospital rooms expedite recovery from severe and refractory depressions. J Affect Disord, 40: 49-51. |
| [72] | Wilson, E. O. (1984). Biophilia. Harvard University Press, Cambridge, Massachusetts. |
| [73] | Ulrich, R. S. (1984). View through a window may influence recovery from surgery. Science, 224(4647), 420-421. |
| [74] | Ulrich, R. S., Lundén, O., & Eltinge, J. L. (1993). Effects of exposure to nature and abstract pictures on patients recovering from heart surgery. Paper presented at the Thirty-Third Meetings of the Society for Psychophysiological Research, Rottach-Egern, Germany. Abstract published in Psychophysiology 30(Suppl. 1), 7. |
| [75] | Brown, C. J., Chen, A. C. N., & Dworkin, S. F. (1989). Music in the control of human pain. Music Therapy, 8(1), 47-60. |
| [76] | Daveson, B. A., & Kennelly, J. (2000). Music therapy in palliative care for hospitalized children and adolescents. Journal of Palliative Care, 16, 35-38. |
| [77] | Weber, S., Nuessler, V., & Wilmanns, W. (1997). A pilot study on the influence of receptive music listening on cancer patients during hemotherapy. International Journal of Arts Medicine, 5(2), 27-35. |
| [78] | Beck, S. L. (1991). The therapeutic use of music for cancer-related pain. Oncology Nursing Forum, 18: 1327-1337. |
| [79] | Magill-Levreault, L. (1993). Music therapy in pain and symptom management. Journal of Palliative Care, 9, 42-48. |
| [80] | O’Callaghan, C. C. (1996). Pain, music creativity, and music therapy in palliative care. Complementary Medicine International, 3(2), 43-48. |
| [81] | Williamson, A., & Hoggart, B. (2005). Pain: a review of three commonly used pain rating scales. Journal of clinical nursing, 14(7), 798-804. |
| [82] | Choinière, M. and Amsel, R. (1996). A visual analogue thermometer for measuring pain intensity. Journal of Pain and Symptom Management, 11(5): 299-311. |
| [83] | Melzack, R. (1975). The McGill Pain Questionnaire: Major properties and scoring methods. Pain, 1(3): 277-299. |
| [84] | McGrath, P. J., Johnson, G., Goodman, J. T., Schillinger, J., Dunn, J., & Chapman, J. (2003). Children’s Hospital of Eastern Ontario Pain Scale. Assessing Children’s Well-Being: A Handbook of Measures, 28(3), 38. |
| [85] | Taal, L. A., & Faber, A. W. (1997). The burn specific pain anxiety scale: introduction of a reliable and valid measure. Burns, 23(2), 147-150. |
APA Style
Kader, S. (2025). Pain and Environmental Stimuli: A Review on Research Methods, Instruments, and Findings. American Journal of Applied Psychology, 14(1), 29-51. https://doi.org/10.11648/j.ajap.20251401.14
ACS Style
Kader, S. Pain and Environmental Stimuli: A Review on Research Methods, Instruments, and Findings. Am. J. Appl. Psychol. 2025, 14(1), 29-51. doi: 10.11648/j.ajap.20251401.14
AMA Style
Kader S. Pain and Environmental Stimuli: A Review on Research Methods, Instruments, and Findings. Am J Appl Psychol. 2025;14(1):29-51. doi: 10.11648/j.ajap.20251401.14
@article{10.11648/j.ajap.20251401.14,
author = {Sharmin Kader},
title = {Pain and Environmental Stimuli: A Review on Research Methods, Instruments, and Findings
},
journal = {American Journal of Applied Psychology},
volume = {14},
number = {1},
pages = {29-51},
doi = {10.11648/j.ajap.20251401.14},
url = {https://doi.org/10.11648/j.ajap.20251401.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajap.20251401.14},
abstract = {Pain, as a critical health outcome, has been extensively studied across various disciplines. However, the role of environmental stimulation in reducing patients' perceptions of pain in healthcare settings is a relatively emerging area of research. Recent studies have explored the use of environmental stimuli, such as light, nature, music, and virtual reality, as sources of distraction to alleviate pain during medical procedures. This study aims to examine the research objectives, methodologies, and findings of empirical studies in this domain, addressing the following questions: What types of research designs and methods have been employed? What instruments have been used to measure pain? What are the key findings from these studies? A systematic literature search was conducted across four major databases—PsycINFO, PubMed, Wiley Online Library, and Google Scholar—using eight keywords: ‘pain,’ ‘environment,’ ‘light,’ ‘nature,’ ‘sound,’ ‘music,’ ‘virtual reality,’ and ‘video.’ Studies were included if they were empirical, published after 2000, measured pain as a health outcome, and emphasized environmental factors. A total of 53 studies met these criteria. An analytical matrix was developed to categorize studies based on research objectives, design, sample size, methodology, and pain measurement tools. The findings were synthesized into four major themes: environmental interventions, research designs, pain measurement techniques, and outcomes. Environmental contexts included exposure to natural light (two studies), sounds of nature (one study), combined view and sound of nature (one study), music therapy (21 studies), and virtual reality (29 studies). Of the selected studies, 44 employed randomized controlled trials, eight used quasi-experimental designs, and one was descriptive correlational. Pain was measured using a variety of validated instruments, and the study provides a comprehensive list of these tools, detailing their strengths and limitations. This article offers valuable insights for future research by identifying methodological gaps, suggesting research designs that incorporate environmental stimuli, and recommending appropriate pain measurement instruments. Additionally, graphical representations of research processes, pain scale administration guidelines, and pain rating scale comparisons are included to assist researchers in designing rigorous studies. These resources are particularly useful for planning randomized controlled trials or quasi-experiments to investigate the effectiveness of environmental stimulation as a distraction for reducing pain perception in healthcare settings.
},
year = {2025}
}
TY - JOUR T1 - Pain and Environmental Stimuli: A Review on Research Methods, Instruments, and Findings AU - Sharmin Kader Y1 - 2025/02/20 PY - 2025 N1 - https://doi.org/10.11648/j.ajap.20251401.14 DO - 10.11648/j.ajap.20251401.14 T2 - American Journal of Applied Psychology JF - American Journal of Applied Psychology JO - American Journal of Applied Psychology SP - 29 EP - 51 PB - Science Publishing Group SN - 2328-5672 UR - https://doi.org/10.11648/j.ajap.20251401.14 AB - Pain, as a critical health outcome, has been extensively studied across various disciplines. However, the role of environmental stimulation in reducing patients' perceptions of pain in healthcare settings is a relatively emerging area of research. Recent studies have explored the use of environmental stimuli, such as light, nature, music, and virtual reality, as sources of distraction to alleviate pain during medical procedures. This study aims to examine the research objectives, methodologies, and findings of empirical studies in this domain, addressing the following questions: What types of research designs and methods have been employed? What instruments have been used to measure pain? What are the key findings from these studies? A systematic literature search was conducted across four major databases—PsycINFO, PubMed, Wiley Online Library, and Google Scholar—using eight keywords: ‘pain,’ ‘environment,’ ‘light,’ ‘nature,’ ‘sound,’ ‘music,’ ‘virtual reality,’ and ‘video.’ Studies were included if they were empirical, published after 2000, measured pain as a health outcome, and emphasized environmental factors. A total of 53 studies met these criteria. An analytical matrix was developed to categorize studies based on research objectives, design, sample size, methodology, and pain measurement tools. The findings were synthesized into four major themes: environmental interventions, research designs, pain measurement techniques, and outcomes. Environmental contexts included exposure to natural light (two studies), sounds of nature (one study), combined view and sound of nature (one study), music therapy (21 studies), and virtual reality (29 studies). Of the selected studies, 44 employed randomized controlled trials, eight used quasi-experimental designs, and one was descriptive correlational. Pain was measured using a variety of validated instruments, and the study provides a comprehensive list of these tools, detailing their strengths and limitations. This article offers valuable insights for future research by identifying methodological gaps, suggesting research designs that incorporate environmental stimuli, and recommending appropriate pain measurement instruments. Additionally, graphical representations of research processes, pain scale administration guidelines, and pain rating scale comparisons are included to assist researchers in designing rigorous studies. These resources are particularly useful for planning randomized controlled trials or quasi-experiments to investigate the effectiveness of environmental stimulation as a distraction for reducing pain perception in healthcare settings. VL - 14 IS - 1 ER -
Department of Construction Management and Interior Design, Estopinal College of Architecture and Planning, Ball State University, Muncie, USA
Biography: Sharmin Kader, Ph.D., is an assistant professor at Ball State University. She is an architectural designer and researcher. Sharmin received her doctoral degree in architecture from the University of Kansas in 2016 and her master’s degree in construction management from Texas A&M University. She worked as a postdoctoral research scholar at Kent State University in the healthcare design program. She has received numerous awards and has been published in many venues. She also served as a journal article reviewer, a reviewer of conference proposals, a juror of international awards, and an editor of books or proceedings. She served as the Chair of the Board of the Environmental Design Research Association (EDRA) in 2020-22. She was the Chair of the education committee of the Nursing Institute for Health Design in 2023. Currently, she is serving as a co-chair of the sub-committee of the Academy of Architecture for Health (AIA-AAH).
Research Fields: Sharmin Kader: healthcare facility design, post-occupancy evaluation, hospice care environment, environmental gerontology, and environment for higher education.


Figure 1. Visual Analog Scale (VAS).

Figure 2. Numerical Rating Scale (NRS)
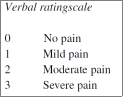
Figure 3. Verbal Rating Scale (VRS).

Figure 4. Graphic Rating Scale (GRS).
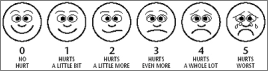
Figure 5. Faces Pain Scale (FPS).

Figure 6. Faces Pain Scale-Revised (FPS-R).
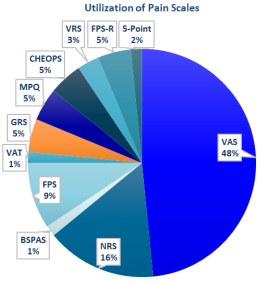
Figure 7. Utilization rate of pain scales in the selected studies.
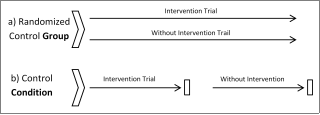
Figure 8. Two types of randomized control trial process.
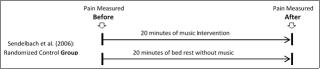
Figure 9. Pain scale administration - before and after.
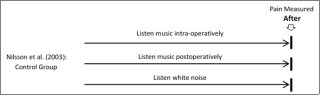
Figure 10. Pain scale administration - only after the procedure.

Figure 11. Pain scale administration - only after the procedure.

Figure 12. Pain scale administration - periodically during process.

Figure 13. Pain scale administration - frequently during process.

